
Introduction
The acardiac twin or TRAP sequence is a rare complication of mono zygotic multiple pregnancy. TRAP sequence is characterized by having one normally formed “pump” twin and one acardiac (congenital absence of heart) “perfused” twin. The normal twin works as the donor and has an increased arterial perfusion pressure whereas the acardiac twin receives deoxygenated blood pumped by its co twin due to reversal of blood flow in the umbilical artery.1
The etiopathogenesis of acardiac anomaly is explained by the presence of an arterio -arterial anastomosis or by organ dysmorphogenesis2 Cardiac dysmorphogenesis is developmental defect in organogenesis, a “ cardiac regression sequence ”. The arterio-arterial anastomosis is characterized by the reversed blood flow from umbilical artery of the pump twin into the umbilical artery of the perfused twin due to sharing of a common placenta and abnormal placental vascular anastomoses between the twins.4, 3
The pump twin is at risk of development of cardiac failure, intra uterine growth retardation, polyhydramnios or even Intra uterine death due to reversal of flow. So the aim is early diagnosis with intensive monitoring of pregnancy or interventions as and when necessary.
When acardiac twin is smaller than the pump twin (< 70% of the pump twin weight) and there is no sign of cardiac decompensation in pump twin, conservative management is the best option; to prevent premature birth and to avoid complications of interventions.5
Case Report
This is a case of a 24 year old gravida 2 para1 live1 with spontaneous conception at 35 weeks of gestation. Ultrasonographic finding was suggestive of twin pregnancy with intrauterine fetal deathand anencephaly of one twin; and a second live twin of 28 weeks 1 day. There was no previous obstetric ultrasound or fetal anomaly scans available with the mother.
The mother was found to be normal on general examination with stable vital parameters.
Obstetric examination
Fundal height 34 weeks, multiple fetal parts felt with a single fetal heart sound audible.
Ultrasonography
Monochorionic twin pregnancy with the pump twin having normal fetal anatomy consistent with 25weeks and 4days [Figure 1 A.]; whereas twin B (the acardiac twin) had grossly abnormal anatomy [Figure 1 B]. Fe tal skull, thorax, upper limbs were absent in the twin B. No identifiable cardiac structures and cardiac activity were noted. Only lower limbs were present with femur length of 3.78cms corresponding to 22 weeks 1 day.
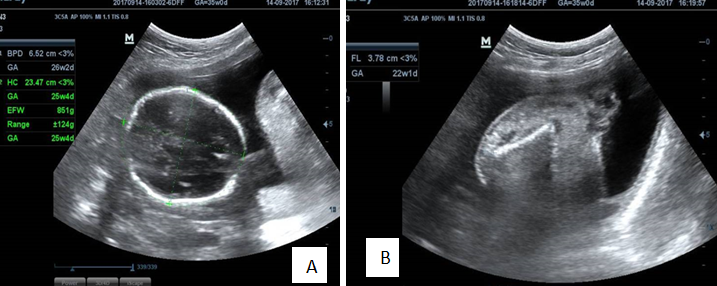
Estimated fetal weight was 851 g for the pump twin. There was no pericardial effusion or congestive heart failure found. On doppler study ; umblical artery was S/D ratio-3.49 and PI-1.20. Intensive monitoring of the pump twin by serial growth scans and doppler studies were done.
Interval growth scan of pump twin after 3 weeks was consistent with 28 weeks 4 days with an estimated fetal weight of 1081 grams. Doppler study showed normal hemodynamics in pump twin (umblical artery S/D ratio-3.32and PI-1.23). Interval growth of the acardiac twin showed femur length of 4.19 cm;which was corresponding to 23 weeks 4days.
A week later, the patient presented with complains of decreased fetal movement. Urgent ultrasonography with colour doppler was suggestive of absent end diastolic flow in uterine artery of pump twin. The estimated fetal weight of the Pump twin at that time was 1179 grams.
Parents were counselled regarding termination of pregnancy in view of decreased fetal movements and abnormal doppler study findings of absent diastolic flow. Appropriate steps for lungs maturation and neuroprotection of fetus were taken.
Emergency caesarean section was done and a preterm male live baby was delivered with birth weight of the 1110grams and no obvious congenital malformation. APGAR score of the newborn was 9 and 10 at 1 and 5 minutes, respectively. Twin B was acardiac and weighed 270grams with placental membranes directly attached to the umbilical area (umbilical cord was absent). Only lower limbs & lower part of abdomen were developed. External genitals were also poorly developed. On examination, placenta was diamniotic monochorionic and weighed 390g rams. Histopathology examination showed a monochorionic diamniotic placenta. Sections examined from umbilical cord, showed presence of three vessels ; and section examined from the membran es showed chorion & amnion with focal lymphocytic infiltration & fibrin deposition. Twin A was under intensive care for 26 days and the screening tests for congenital anomalies were negative.

Discussion
Vascular anastomosis in placenta of monochorionic twin pregnancy may cause serious complications. TRAP sequence or acardiac twin results from large arterio-arteriolar anastmaosis. This condition was first described by Benedettiin the 16th century6 with an incidence of about 1 per 35,000 births.7
TRAP sequence was defined by Van Allen et al. in 1983,8 as a reversed perfusion from pump to acardiac twin via single anastomosis. This anastomosis can be either vein-to-vein or arterial-to-arterial, between the two cords or indirectly through the chorionic plate. Acardiac twin loses direct vascular connections with the placental villi and receives blood from pump twin through umbilical artery and the venous blood exits through umbilical vein.9
The acardiac twin is perfused with hypoxic blood; which is preferentially to the lower part of body. Hence the acardiac twin has well developed lower part of the body with100% mortality. Majority of the pump twins are anatomically normal, but their survival rate is only about 50% due to associated complications like heart failure, polyhydramnios or prematurity.8 In some cases, anomalies may be observed in the pump twin like cardiogenic defects, gastroschisis and skeletal abnormalities.10
Acardiac twin is classified according to the degree of morphological maldevelopment.11
Acardius-acephalus – The acardiac twin has no cephalic development. Head and upper extremities are absent. This is the most common type.
Acardius-anceps – The acardaic twin has cranialstructures and neural tissue development. The body and upper extremities are present. This is a highly developed form of acardiac twin.
Acardius-acormus – In this, the twin has cephalic structure, but no trunk al structures are present. The umbilical cord is attached to the head. This is the rarest form of the acardia.
Acardius amorphous – In this the acardaic twin has the most severe malformation with nodistinguishable cephalic or truncal structure. This is leastdeveloped form and has no recognizable human structures. This differs from teratomasonly by its attachment to an umbilical cord.
Management
Regularsonographicsurveillances should be initiated to assess the weight ratio of twins and signs of development of congestive cardiac failure and hydramniosin pump twin should be monitored. Weight can be estimatedby comparing the ratio of the abdominal perimeter of the acardiac and pump twins, or by using the standardprolate ellipsoid formula (ie. length of acardiac x abdominal diameter divided by 2).12
The prognosis of conservative management is excellent if the estimated weight of the acardiac twin is less than one fourth of the pump twin. This risk is 100% when the weight of the acardiac twin exceeds 70% than that of the pump twin.12 This is due to increased perfusion demands of the relatively large acardiac twin. In such cases, the donor twin (pump twin) has to maintain its own blood flow and also of the acardiac twin, and thus may lead to decompensation of the pump twin heart leading to failure.
At this point, some form of minimally invasive intervention is warranted to interrupt the vascular communication between the twins. Historically, uterotomy and removal of the acardiac twin is present in literature.13 Later, fetoscopic coagulation of placental anastomosis and endoscopic ligation of umbilical artery of acardiac twin have been described.14, 13
Cord occlusion has been attempted by ultrasound-guided injection of thrombogenic materials into the umbilical circulation of the acardiac twin. Ligation of the umbilical cord, laser coagulation, bipolar diathermy, and monopolar diathermy are the other available options to interrupt the vascular anastomosis between the two twins.15
Intrafetal ablation with alcohol, interstitial laser, monopolar diathermy, and radiofrequency ablation have also been performed in such cases.15 In comparison to the more invasive techniques for umbilical artery occlusion; intra fetal ablation is more effective, safer and technically easier to perform.16 Greater than 90% survival of the pump twin is seen in TRAP Sequence treated with radiofrequency ablation.16 Recently, high intensity focused ultrasound (HIFU) has been used for occlusion of the blood flow in the acardiac twin.17
A study conducted by Moore et al.18 reviewed the perinatal courses of 49 acardiac twin pregnancies, showed perinatal mortality to be 55% and the mortality was primarily associated with prematurity. When the twin-weight ratio was above 70%, the incidenceof pump-twin congestive heart failure was 30%, hydramnios was 40%; and preterm delivery was 90%. Whereasthe rates of congestive heart failure, hydramnios and preterm delivery were 10%, 30%, and 75 %, respectively, when the twin weight ratio was less than 70%.
Conclusion
In monochorionic twin pregnancies with acardiac twin; risk of mortality of pump twin is very high. Early diagnosis,proper ultrasound surveillances for monitoring and treatment (either conservative or invasive) for the pump twin at right time is required to improve perinatal outcome. Thorough and proper monitoring, accurate diagnosis and timely interventions with co-operation and awareness from patients may help in improving the outcomes in such cases.