
Introduction
Ovarian torsion is a phenomenon describing a complete or partial rotation of the adnexa around its own vascular axis or pedicle. Establishing the fact that, the precise etiology for torsion remains to be unknown, however, the predisposing factors are moderate size cyst, free mobility and a long pedicle. Torsion of ovarian tumours are chiefly seen in reproductive age group. An enormous number of cases are presented during pregnancy (22.7%) than when compared with non-pregnant (6.1%) women.1 During pregnancy, there happens to be a 5 fold increased risk of ovarian torsion, with an incidence accounting up to an approximate 5 per 10,000 pregnancies.2 The incidence is greater at gestational age of about 10–17 weeks with ovarian masses greater than 4 cm.
The commonly seen benign masses during pregnancy include conditions such as serous cystadenoma benign cystic teratomas and functional ovarian cysts. During an event of complete torsion, there is venous and lymphatic blockade which in turn leads venous congestion following which stasis, haemorrhage and necrosis occur. Here we present a case report of an ovarian torsion in first trimester of pregnancy.
Case Presentation
A 28-year-old women who is Gravida 4 Para 0 Abortion 3 with 10 week 2 days gestation conceived after infertility treatment (ovulation induction) presented to casualty with C/O pain abdomen, sudden in onset, non-radiating type with no relieving factors and with 4 bouts of vomiting. While examining, it was found that she was afebrile, with her vitals being stable. Proceeding to abdominal examination, abdomen was soft, diffuse tenderness was present, which was elicited more in right iliac fossa, there was diffuse guarding with no rebound tenderness. Moving on to speculum examination, external OS was found to be closed with no evidence of bleeding. The uterus was 10-12 weeks palpable. Also, on bimanual examination, there seemed to be right adnexal fullness and tenderness.
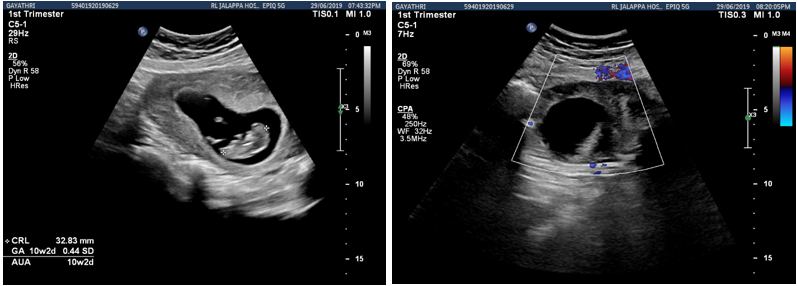
Later on, the pelvic Ultrasonography revealed a single live intrauterine gestation corresponding to 10 weeks 2 days with good fetal cardiac activity. It also revealed, a bulky right ovary measuring [8.9cmx7.5cmx 5.3cm] with cystic lesions, with no visible arterial/venous flow in the right ovary, which contributed to the conclusion of a right ovarian torsion.
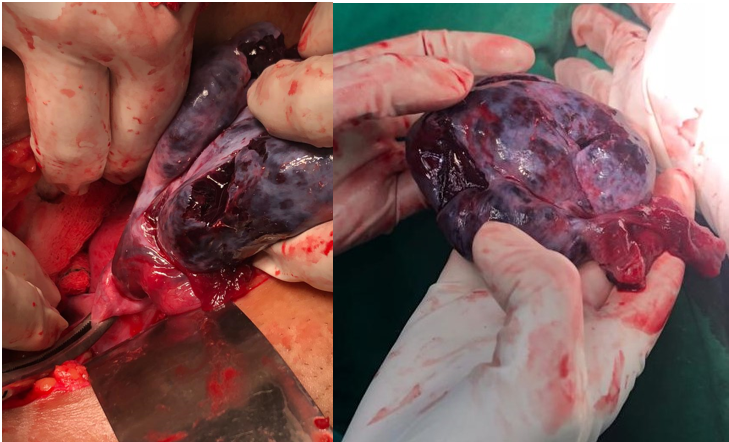
Patient was given Inj Hydroxy progesterone caproate 500 mg IM preceding the surgery. After obtaining a completely informed consent, the patient went through an exploratory laparotomy under spinal anaesthesia using a pfannensteil incision. A right sided irregularly enlarged, necrosed, haemorrhagic ovary of 10cm x 5cm without Normal ovarian tissue. Free fluid of 5cc present in pouch of Douglas. Right ovarian pedicle torsion of 2 ½ turns was present, which was released. Right oophorectomy done.
Patient withstood the procedure well. There were no complications witnessed postoperatively. Upon her discharge, she was advised to consume oral Progesterone till 12 weeks of gestation and was asked for regular follow up. Histopathological report revealed, a serous cystadenoma of right ovary with torsion. Patient was later on followed up with obstetric scan which seemed to be normal.
Discussion
In a non-pregnant women, ovarian torsion may not be a common cause of acute abdominal pain, but this does not hold true when it comes to pregnant women. Unilateral benign cysts are more frequently associated with reproductive age group.3 Nearly 70% of all serous cystadenomas are found to be benign tumours, 5–10% have a borderline malignant potential and 20–25% are found to be malignant.
Cysts lesser than 6 centimetres in diameter and associated with benign features on ultrasonography can be managed conservatively as majority of them undergo spontaneous resolution. Cysts greater than 10 centimetres in diameter are typically excised, as they escalate the risk of malignancy, rupture or torsion of the cyst. Nonetheless, there occurs to be a controversy in the management of the cysts which occur between 5-10 cms. The cysts that comprise features like septae, nodules, papillary excrescences or solid components, the decision for resection can be made. On the Contrary, the simple cysts, have an expectant management which includes serial ultrasound surveillance. Nevertheless, they may require an emergency exploratory laparotomy if torsion, infarction or rupture arises, which is seen in about 50% cases.4 It is also observed that torsion of an ovary that gets stimulated during procedures like IVF/IUI is not very frequent occurrence. This fact does not rule out the possibility in a women presenting with acute abdominal pain who underwent ovulation induction for IUI or IVF. Delaying the diagnosis and appropriate management would follow ischemic necrosis of ovary.5
Ultrasonography (USG) happens to be the diagnostic modality of choice. USG more so often reveal an unilateral ovarian enlargement that could present as a solid, cystic, or even complex, with / without collection of fluid in the recto-uterine pouch. The Colour Doppler sonography, depicts an enlarged ovary devoid of parenchymal perfusion.6 CT and MRI can be used when USG findings seem inconclusive. The gold standard modality to treat and confirm ovarian torsion is surgery which could either be laparoscopy or laparotomy. During surgery, assessing the ovarian viability to preserve its function is of utmost importance. The only method to determine the viability of torsioned ovary during surgery is by gross visual inspection. The conventional method, where dark and enlarged ovaries may have vascular and lymphatic congestion, they may seem nonviable.7 If the ovarian tissue is not necrosed, detorsion could be considered. The decision of proceeding for surgery all through the pregnancy is enigmatic. Meanwhile, the well-being of both mother and foetus must be considered. Then again, the risk of any surgery to a pregnant will depend on gestational age. On those lines, during first trimester, when the ovarian torsion is the most frequent, the risk observed for the fetal loss is tiniest with the use modern anaesthetic technique.8
Conclusion
Ovarian torsion is an emergency gynaecological condition, which unfortunately can occur during pregnancy as well. Fortunately, it can be diagnosed with its typical clinical presentation alongside ultra-sonographic evidence of an unilaterally enlarged adnexal mass. Although, the management options for an adnexal torsion, irrespective of the gestational age is limited to surgery, it is performed for the betterment of maternal and perinatal outcome.