
Introduction
Abnormal uterine bleeding is any variation in the normal menstrual cycle, Includes: changes in frequency, duration and amount of blood loss during or in between the cycles.1
Approximately 70% of all gynecological consultations in perimenopausal and postmenopausal women are for abnormal uterine bleeding. There complaints may significantly affect the quality of life and lead to surgical intervention.2
Abnormal perimenopausal or postmenopausal bleeding is associated with endometrial carcinoma in approximately 10% of cases and is considered to be caused by endometrial neoplasia until proven otherwise.3, 4
Approximately 90% of women with endometrial carcinoma present with vaginal bleeding.
In 18% to 40% of women, benign focal lesions, such as endometrial polyps and fibroids, are common. Although PMB is most commonly due to other conditions, it is essential to exclude endometrial carcinoma.5
TVS is an inexpensive, non-invasive, easily available and a convenient method to assess the uterine pathology.
It is recommended as the 1st line diagnostic tool for assessing uterine pathology in perimenopausal age women presenting with abnormal uterine bleeding.2, 4
Drawbacks include- limited field of view, obscuration of pelvis by bowel gas and its dependence on the skill expertise.6
In the pelvis, MRI appears to have a 91-93% overall precision for characterising benign and malignant lesions particularly when contrast techniques are used.5, 7, 8
Magnetic resonance imaging because of its high resolution and multi planar imaging and its capability to characterize multiple lesions is becoming the modality of choice to assess the pathologies of pelvis.9
Classification of lesions10
Lesions of myometrium - Leiomyoma and adenomyosis.
Lesions of endometrium - Endometrial polyp, endometrial hyperplasia and endometrial carcinoma.
Lesions of cervix - Cervical carcinoma, cervicitis.
Adnexal lesions - Hydrosalpinx, hematosalpinx, pyosalpinx, simple. ovarian cysts, hemorrhagic ovarian cyst, endometriotic cysts and dermoid cysts.
Materials and Methods
Sample size
40 patients in perimenopausal age group with complain of abnormal uterine bleeding attending OPD at C.U. Shah medical college and hospital.
All patients were subjected to TVS and MRI examination.
Final correlation with histopathology was done wherever it was acquired.
TVS was performed on Affinity Philips 70G transvaginal transducer.
Magnetic resonance imaging of pelvis was performed with 1.5T SIEMENS machine.
Clinical history was taken, TVS was done and the findings were noted.
Informed consent was taken from all patients & MRI was done using standard protocol.
All patients were followed up when it was possible.
Histopathology reports were collected when necessary from patients who underwent surgery or biopsy.
Result
Among 40 females, majority of them were in pre menopause period 25 (62.5%) and the rest in the post menopause period 15 (37.5%).
Table 1
Distribution of pre and post menopause study participants
|
|
Frequency |
Percent |
|
Pre menopause |
25 |
62.5 |
|
Post menopause |
15 |
37.5 |
|
Total |
40 |
100 |
Among 40, majority were diagnose fibroids 14 (37.5%), adnexal lesions 11 (27.5%), carcinoma of cervix 5 (12.5%), endometrial lesions 6(12.5%) and adenomyosis 4 (10.0%).
Table 2
Distribution of cases
|
Number of Cases |
Frequency |
Percent |
|
Fibroids |
14 |
35.5 |
|
Adenomyosis |
4 |
10.0 |
|
Carcinoma of cervix |
5 |
12.5 |
|
Adnexal lesions |
11 |
27.5 |
|
Endometrial lesions |
6 |
15 |
|
Total |
40 |
100 |
Table 2 describes that adnexal lesions start in early age itself (35±2). Endometrial lesions (51±8) and carcinoma of cervix (55±6) were reported mostly in the post menopausal periods. Fibroids (40±5) and Adenomyosis (42±4) were reported in middle age.
Table 3
Comparision of Mean age with final diagnosis
|
Final diagnosis |
Mean Age |
|
Fibroids |
40±5 |
|
Adenomyosis |
42±4 |
|
Carcinoma of cervix |
55±6 |
|
Adnexal lesions |
35±2 |
|
Endometrial lesions |
51±8 |
Table 3 describes that out of 4 cases TVS could detect only 2 as Adenomyosis and other 2 were? Adenomyosis.
This explains that there is significant difference in diagnosing adenomyosis using TVS and MRI.
Table 4
Comparison of TVS findings with MRI findings for Adenomyosis
|
TVS Diagnosis |
MRI Diagnosis |
Total |
|
|
|
Adenomyosis |
Adenomyosis with fibroid uterus |
|
|
? Adenomyosis |
2 |
0 |
2 |
|
? Adenomyosis with fibroid uterus |
0 |
1 |
1 |
|
Adenomyosis |
1 |
0 |
1 |
|
Total |
3 |
1 |
4 |
Among 4 cases of adenomyosis MRI detect all (100%) where in TVS showed only 2 cases as positive.
Sensitivity =50%
Positive likelihood ratio = 0.5
Sensitivity = 60%
Positive predictive value (PPV) = 60%
Positive likelihood ratio = 0.9
Out of 8 cases TVS picked up 3 cases as positives were as HPE picked up all 5 cases of ca cervix. The true positives were 3 and true negatives were 1, there were 2 false negative and 2 false positives by the diagnosing test. There is no significant association detected.
Table 5
Comparison of Ca Cervix diagnosed by TVS with HPE
|
Ca Cervix TVS |
HPE |
||
|
Present |
Absent |
Total |
|
|
Present |
3 |
2 |
5 |
|
Absent |
2 |
1 |
3 |
|
Total |
5 |
3 |
8 |
Out of 8 samples MRI and HPE picked all 5 cases of ca cervix. The true positives were 5 and true negatives were 3. There is significant association detected.
Table 6
Comparison of Ca Cervix diagnosed by MRI with HPE
|
MRI |
Ca Cervix HPE |
||
|
Present |
Absent |
Total |
|
|
Present |
5 |
0 |
5 |
|
Absent |
0 |
3 |
3 |
|
Total |
5 |
3 |
8 |
Out of 16 samples TVS picked up 6 cases as positive whereas HPE picked 6 cases of Endometrial Lesions. The true positives were 4 and true negatives were 8, there were 2 false positives and 2 false negatives by the diagnosing test.
Sensitivity = 66.6%
Specificity = 80%
Positive predictive value (PPV) = 66.6%
Negative predictive value (NPV) = 80%
Table 7
Comparision of endometrial lesions diagnosed by TVS with HPE
|
TVS |
Endo Lesions HPE |
||
|
Present |
Absent |
Total |
|
|
Present |
4 |
2 |
6 |
|
Absent |
2 |
8 |
10 |
|
Total |
6 |
10 |
16 |
Table 8
Comparison of endometrial lesions diagnosed by MRI with HPE
|
MRI |
Endo Lesions HPE |
||
|
Present |
Absent |
Total |
|
|
Present |
5 |
1 |
6 |
|
Absent |
1 |
9 |
10 |
|
Total |
6 |
10 |
16 |
Out of 16 samples MRI picked up 5 cases as positive whereas HPE picked 6 cases of endometrial lesions. The true positives were 5 and true negatives were 9, there were 1 false positive and 1 false negative by the diagnosing test.
Sensitivity = 83.3%
Specificity = 90%
Positive predictive Value (PPV) = 83.3%
Negative predictive value (NPV) = 90%
Table 9
Comparison of number of Fibroid by TVS and MRI
|
TVS |
MRI |
|
|
Single |
Multiple |
|
|
Single |
6 |
3 |
|
Multiple |
NIL |
5 |
There is significant association between TVS and MRI.
Sensitivity =100%
Specificity = 62.5%
Positive predictive value (PPV) = 66.6%
Negative predictive value (NPV) =100%
Table 10
Comparison of frequency of diagnosis of adnexal lesions by TVS and MRI
There is significant association between TVS and MRI.
Among 11 patients TVS diagnosed 4 as complex adnexal cysts, 3 as dermoid, 2 as simple ovarian Cyst, 1 as haemorrhagic cyst and 1 as possibly hydrosalphinx and MRI diagnosed 3 as complex adnexal cysts, 3 as dermoid, 2 as simple ovarian cysts, 2 as haemorrhagic cyst and 1 as hydrosalphinx.
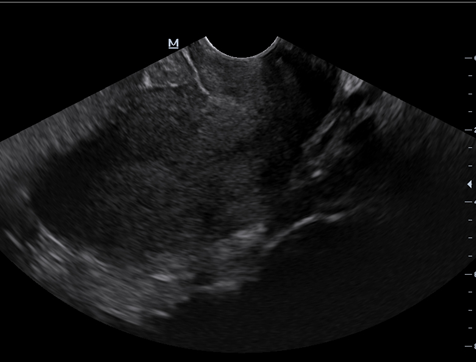
Figure 1
T2 sagittal section of MRI pelvis shows hyperintense areas within the thickened junctional zone representing cystic changes of Adenomyosis







Conclusions
Abnormal uterine bleeding is a common symptom in perimenopausal women. Accurate diagnosis is essential to rule out benign or malignant conditions and provide the most appropriate treatment.2, 4
To characterize, localize and evaluate the number of lesions both benign and malignant along with its staging in pelvic pathologies, MRI is found to be more precise and many a times gold standard in comparison to ultrasound.6, 11
In cases of adenomyosis, MRI turned out to be more accurate in its diagnosis where as ultrasound was found indeterminate in visualizing the junctional zone.12, 13
In cases of fibroids in aiding their number and location, MRI turned out to be more superior than transabdominal and transvaginal ultrasound. In endometrial lesions, TVS can be used as a great screening tool. MRI was found to be crucial in determining myometrial invasion.14
Extent of carcinoma cervix and its invasion to adjacent viscera was found to be superior in MRI compared to ultrasound.
In the adnexa lesions, characterization and differentiation of various types of lesions, TVS was less specific in contrast to MRI.
Finally, we conclude that TVS lacks specificity and sensitivity in relation to MRI but acts as a better screening tool in evaluation and further management as it is cost effective, easily available and less time consuming. MRI is accordingly a more precise preoperative imaging modality for portraying and distinguishing the distinct features of varied lesions.