- Visibility 161 Views
- Downloads 27 Downloads
- DOI 10.18231/j.ijogr.2022.078
-
CrossMark

Dermoid cyst of ovary: A common pathology with an uncommon presentation
Introduction
Germ cell tumours account for 15-20% of all ovarian tumours, with the bulk of these being mature cystic teratomas.[1] Mature teratoma is the most common germ cell tumour of the ovary, which can strike at any age but is most common in the first two decades of life.[2], [3]
The size, compression, or torsion of this slow-growing lesion, as well as chemical peritonitis caused by an intraabdominal leak of cholesterol-laden material, are the most common clinical manifestations.
We present a case of dermoid ovarian cyst with a peculiar gross appearance, despite the fact that it is fairly common in frequency and presentation.
Case Report
A 30-year-old lady presented to the Gynaecology OPD with pain abdomen. Her vital statistics were stable upon testing. There were no abnormalities found on a systemic evaluation. Her most recent labour was two years earlier, and all of her deliveries had been vaginal. A movable mass, the size of a 24-week uterus, was discovered during an abdominal check. A speculum examination of the cervix and vaginal area revealed no abnormalities. A cystic and movable mass anterior to the uterus was discovered during a vaginal examination. The patient was admitted and laboratory investigations were conducted. Her blood cell count and biochemical markers were both within normal limits. CA125 was found to be 16 IU/ml (normal: 0-35IU/ml) in a preoperative tumour marker assay. Ultrasonography indicated a massive cystic mass in the right adnexa including several floating, highly echogenic spherical masses, which were suggestive of a right ovarian cyst (dermoid cyst). The other ovary and uterus appeared normal, and there was no tumour in the upper abdomen. The patient was transported to the operating room for a laparotomy. When the abdomen was opened, a massive right ovarian cyst measuring (12x10) cm was discovered. It was not adherent to any other organs. The right ovary did not show any evidence of torsion. The uterus, left tube, and ovary were all in good shape. Salpingo-oophorectomy on the right side was performed.
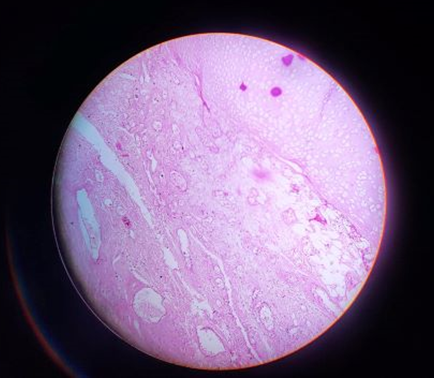
The specimen was submitted to the Department of Pathology for histopathological examination. Cut section of the cystic mass showed multiple (about 50) yellow-white sebaceous balls of varying size inside the cyst ([Figure 1]). No calcified mass or tooth element was found on gross examination. Multiple sections from the cyst wall were submitted for histopathological processing. The histopathological features were consistent with benign cystic teratoma ([Figure 2]). The patient's post-operative recovery went smoothly. In the one-year post-operative follow-up, there was no evidence of recurrence.

Discussion
Benign cystic teratomas are formed from the primitive germ cells of the embryonic gonad and are among the most prevalent ovarian neoplasms (15 percent -25 percent). They are most common during active reproductive years, are uncommon prior to puberty, and are not uncommon in postmenopausal women. Although they comprise well-differentiated derivatives of the three germ layers[4], [5] ectoderm, mesoderm, and endoderm, ectodermal elements predominate; thus, dermoid cysts are sometimes known as ectodermal cysts. Dermoid cysts are usually hidden unless they grow large enough to generate a palpable abdominal mass or cause pain due to torsion, the most common consequence caused by their long pedicle. On abdominal radiography, certain asymptomatic dermoids with calcification or "tooth" are discovered by chance. Rupture (1%) and malignant transformation (2%) are two more less prevalent problems.[6] On the basis of sonography, CT, or magnetic resonance imaging, a radiologic diagnosis of cystic teratoma can be achieved quickly. The variety and prevalence of internal contents apparently account for the spectrum of sonographic appearances because an ovarian tumour may contain a high number of identifiable tissues, including matted hair, well-formed teeth, and semisolid sebaceous material. On sonography, however, there was no calcification or tooth-like structure in our case. Only a few cases of cystic teratomas with several movable spherical masses were discovered in the literature. They have been discovered in the ovary,[7], [8] retroperitoneum[9] and mediastinum.[10] The nodules in a cystic teratoma of the ovary comprised of sebum waste with skin squames and hair,[8] whereas mobile globules in a mature cystic teratoma of the mediastinum consisted of paste-like material, fat, and hair.[10] Fat accumulation was observed around hair tissue in a retroperitoneal mature cystic teratoma;[9] these spherical entities were dubbed intracystic fat balls.[7], [9] Spherical lumps in our patient were made up of paste-like substance and fat, with some including hair. Multiple spherical, floating, and echogenic fat balls were detected on sonography within the huge anechoic cyst. Multiple spherules floating within a pelvic cystic tumour have not been seen in other tumours, according to Kawamoto et al; [11] thus, this morphology is pathognomonic for a cystic teratoma. In conclusion, unexpected accompanying features of a mature cystic teratoma may provide diagnostic problems on certain occasions. Cystic teratomas with numerous mobile spherules or globules have been documented in a small number of cases. Therefore, a strong suspicion in radiology with floating spherical balls supported by a histopathological diagnosis would avoid confusion in clinical diagnosis and pave the way for a better management in patients.
Source of Funding
None.
Conflict of Interest
None.
References
- A Talerman. Germ cell tumors of the ovary. Blaustein's Pathology of the Female Genital Tract 1994. [Google Scholar]
- JS Berek, NF Hacker. . Pathology, practical Gynecologic Oncology 2004. [Google Scholar]
- PJ Disaia, WT Creasman, PJ Disaia, WT Creasman. Germ cell, stromal, and other ovarian tumors. Clinical Gynecological 2002. [Google Scholar]
- ER Novak, JD Woodruff. . Novak's Gynecologic and Obstetric Pathology with Clinical and Endocrine Relations . [Google Scholar]
- RE Scully. Germ cell tumors. In: Tumors of the Ovary and maldeveloped Gonads. Atlas of Tumor Pathology . [Google Scholar]
- RJ Kurman. . Blaustein's Pathology of the Female Genital Tract 1994. [Google Scholar]
- Y Muramatsu, N Moriyama, K Takayasu, S Nawano, T Yamada. CT and MR imaging of cystic ovarian teratoma with intracystic fat balls. J Comput Assist Tomogr 1991. [Google Scholar]
- C Otigbah, MO Thompson, DG Lowe, M Setchell. Mobile globules in benign cystic teratoma of the ovary. BJOG 2000. [Google Scholar]
- H Fujitoh, S Akiyosi, S Takoda, K Katsuki, K Okuda. Hepatobiliary and pancreatic imaging: retroperitoneal mature cystic teratoma with a fat ball. J Gastroenterol Hepatol 1998. [Google Scholar]
- PR Hession, W Simpson. Case report: mobile fatty globules in benign cystic teratoma of the mediastinum. Br J Radiol 1996. [Google Scholar]
- S Kawamoto, K Sato, H Matsumoto, Y Togo, Y Ueda, J Tanaka. Multiple mobile spherules in mature cystic teratoma of the ovary. AJR Am J Roentgenol 2001. [Google Scholar]