- Visibility 638 Views
- Downloads 96 Downloads
- Permissions
- DOI 10.18231/j.ijogr.2025.007
-
CrossMark

Oral arginine versus IV fructodex and oral arginine in the treatment of borderline idiopathic oligohydramnios: A randomised comparative study
- Author Details:
-
 Samya Janarthanam
Samya Janarthanam
-
Sendhil Coumary A *
Abstract
Background: Amniotic fluid is a dynamic medium surrounding the fetus in the amniotic cavity. Decreased amniotic fluid volume of less than 8cm is known as Oligohydramnios. Increasing maternal plasma volume and improving uteroplacental perfusion using nitric oxide (NO) donors is thought to increase the AFI. The present study compares the effect oral arginine supplementation with the combined effect of oral arginine and IV Hydration in increasing AFI in patients far from term and its effect on prolongation of duration of pregnancy.
Materials and Methods: The present study was a randomised-comparative, interventional hospital-based study. Pregnant women between 28 to 36 weeks gestation with AFI less than or equal to 8 cm, were recruited and divided into two groups. Group I was treated with oral arginine for 1 week. Group II was treated with oral arginine and IV fructodex and ringer’s lactate solution once a day for 1 week. Patients were followed up weekly, with USG till delivery.
Results: Post-treatment increase in AFI in Group I and II was 0.95 ± 1.11 cm and 1.87 ± 1.22 cm. The duration of prolongation of pregnancy was 4.48 weeks in Group I and 4.24 weeks in Group II.
Conclusion: This study concludes that treatment with Oral Arginine with IV Fructodex produces a higher increase in AFI compared to oral arginine alone, however, this is transient. In both groups the pregnancy outcomes were similar. Continuous oral arginine till delivery may be more efficient and practical treatment modality in borderline oligohydramnios.
Introduction
Amniotic fluid is an active medium that surrounds the fetus in the amniotic cavity. It is one of the vital necessities for good fetal growth and outcome. The equilibrium is preserved by four chief paths, namely, fetal urination, fetal lung fluid secretion, trans-membranous and intramembranous flow and fetal swallowing.[1]
The American College of Obstetricians and Gynaecologists (ACOG, 2011) defines oligohydramnios as either an amniotic fluid index (AFI) of less than 5 cm, or a maximum deepest vertical pocket of less than 2 cm.[2] Oligohydramnios affects 1-4% of normal pregnancies.[3] The term borderline oligohydramnios refers to AFI between 5-8 cm.
When irregularities of AFI occurs in the first half of pregnancy, they are associated with birth defects and pulmonary hypoplasia in the fetus. In the second half, it is usually related to fetal growth restriction.[4], [5] Long-term oligohydramnios may lead to pressure-induced deformities, irregularities of fetal heart rate during labour, cord compression, meconium aspiration, and increased instrumental deliveries. Thus, early detection and treatment of idiopathic oligohydramnios is crucial.
There is a strong association between maternal plasma volume and amniotic fluid volume. Increase in maternal plasma volume is related to polyhydramnios and decrease in plasma volume to oligohydramnios.[5], [6] Amino acids, like L-arginine, are regulators of placental perfusion.
Various methods have been employed to improve AFI, as there is no one typical treatment procedure for isolated oligohydramnios using any modality alone or in combination. Maternal oral or IV hydration therapy, oral and intravenous amino acids have been tried. Maternal IV hydration has been found to directly increase AFI by improving maternal plasma volume.[7] Treatment with oral or IV amino acid has been found to be useful in cases of oligohydramnios with intrauterine growth restriction and pregnancy induced hypertension.[6], [8] Intravenous dextrose solutions act as a source of energy to the fetus and improve AFI by osmotic diuresis in the fetus.
The present study was done to compare the effect of oral arginine with the combined effect of oral arginine and IV fructodex (a dextrose solution) on the increase in AFI, prolongation of pregnancy duration and fetal outcome in patients far from term with borderline, idiopathic oligohydramnios.
Materials and Methods
The present study was a randomised, comparative, interventional study done in the Department of Obstetrics and Gynaecology, in a tertiary care hospital, between the period of January 2019 to June 2020, after obtaining clearance from Institutional Human Ethical Committee. The study was carried out in accordance with the Helsinki Declaration Principles.
All pregnant women between the gestational age of 28 weeks to 36 weeks, with singleton pregnancy, presenting with AFI of 5cm - 8cm in the Outpatient Department of OBG, formed the study population. Pregnancies with fetal anomalies, patients with medical disorders of pregnancy like renal disease, hypertensive disorders, known heart disease and prelabor preterm rupture of membranes (PPROM) were excluded from the study. The sample size was calculated with a prevalence of 3%, α error of 0.05 and β error of 0.2. Sample size was calculated to be 120, sixty in each group. [3]
Informed consent was taken from the recruited women. A detailed history was taken. All pregnant women fitting the inclusion criteria were taken up for the study. Patients were admitted as in-patients and computer-generated block randomisation was done to obtain two study groups. Group I was administered oral arginine 3 grams only, twice daily for one week. Group II was administered oral arginine 3 grams twice daily along with 500 ml of 10% fructodex, which contains 5% dextrose and 5% fructose, and 500ml of ringer’s lactate solution, once daily over four hours, for one week. Both groups were advised to increase oral fluid intake to 2 litres per day. AFI estimation was done after 1 week, followed by weekly follow up till delivery. All ultrasounds were done transabdominally, using LOGIQ P5 model ultrasound machine. After the treatment period of one week, if liquor volume improves or if it continues to remain the same, both the groups were asked to continue oral arginine 3 grams twice daily till termination of pregnancy. If there was no improvement or if there was a decline, women were counselled regarding continuation or termination of pregnancy as per department protocol. Study was terminated once sample size was met.
Patients in both the groups were followed up till delivery. The primary outcomes noted were increase in AFI after treatment with oral arginine alone in group I, the increase in AFI after combined treatment with oral arginine and intravenous fructodex in group II and a comparison of the AFI between the two groups after treatment.
Secondary outcomes noted were gestational age at delivery, AFI at delivery, baby weight at delivery, mode of delivery, APGAR of baby and the need for NICU care.
Data was collected in excel sheet and analysed using SPSS software (version 17). Quantitative variables were analysed using mean, standard deviation and independent T test. Qualitative variables were analysed as percentage and using Chi Square test. p value of <0.05 was taken as statistically significant.
Results
Post-treatment increase in AFI in Group I was 0.95 ± 1.11 cm and in Group II, it was 1.87 ± 1.22 cm. Both groups had significant increase in AFI after 1 week of treatment. Group II had a higher average increase in AFI than Group I by 0.94 cm and this was found to be statistically significant (p value 0.001). In Group I, the pregnancy was prolonged for an average period of 4.48 weeks and in Group II, it was prolonged for an average of 4.24 weeks. The duration of prolongation of pregnancy was found to be significant in both the groups (p value 0.001). No significant findings were seen in terms of fetal weight gain, mode of delivery, APGAR at 5 minutes and NICU admissions.
|
Variables |
Group I |
Group II |
|
Parity PRIMI |
33 (55%) |
45 (75%) |
|
MULTI |
27 (45%) |
15 (25%) |
|
Mean Gestational Age At Recruitment (In weeks) |
33.59 ± 2.06 |
33.55 ± 2.09 |
|
Mean Gestational Age At Delivery (In weeks) |
38.07 ± 1.09 |
37.79 ± 1.47 |
|
Average increase in duration of pregnancy (In weeks) |
4.48 (3.88 to 5.071) (p value <0.001) |
4.24 (3.59 to 4.89) (p value <0.001) |
|
Mean increase in fetal weight (Kgs) |
0.72 (0.61 to 0.84) |
0.72 (0.59 to 0.86) |
|
Mode of Delivery |
22 vaginal/ 38 LSCS |
29 vaginal/ 31 LSCS |
|
APGAR < 8/10 |
2 |
4 |
|
Groups |
AFI At Start of Treatment |
AFI at end of Treatment |
Mean Increase in AFI |
AFI at Delivery |
Mean Difference in AFI |
|
Group I |
7.52 ± 0.88 |
8.47 ± 1.84 |
0.95 ± 1.11 (p value <0.001) |
7.23 ± 1.98 |
1.23 ± 1.97 (p value <0.001) |
|
Group II |
6.74 ± 1.31 |
8.65 ±1.54 |
1.87 ± 1.22 (p value <0.001) |
6.66 ± 2.10 |
1.99 ± 2.15 (p value <0.001) |
Discussion
Amniotic fluid is a dynamic medium that surrounds the fetus in the amniotic cavity. It has many functions like protecting the fetus, allowing for development of musculoskeletal system, gastrointestinal tract development and normal fetal lung development through fetal swallowing.
Normal AFI is defined as between 5 to 24 cm. An AFI between 5 and 8 cm is considered as low normal (borderline oligohydramnios), and less than 5cm is considered as severe oligohydramnios. Oligohydramnios affects 1-4% of normal pregnancies.[9] There is a strong correlation between maternal plasma volume and amniotic fluid index. Increasing maternal plasma volume is thought to increase AFI.[2] Improving uteroplacental perfusion using nitric oxide (NO) donors is another pathway to improve AFI.[10]
The present study was done to compare the effect of oral arginine alone with oral arginine and intravenous fructodex on AFI in idiopathic borderline oligohydramnios.
In studies done by Hebbar et al and by Soni et al, women with antenatal risk factors which are known causes of gestational hypertension and IUGR were included.[7], [11] In the present study, such causes were excluded before recruitment.
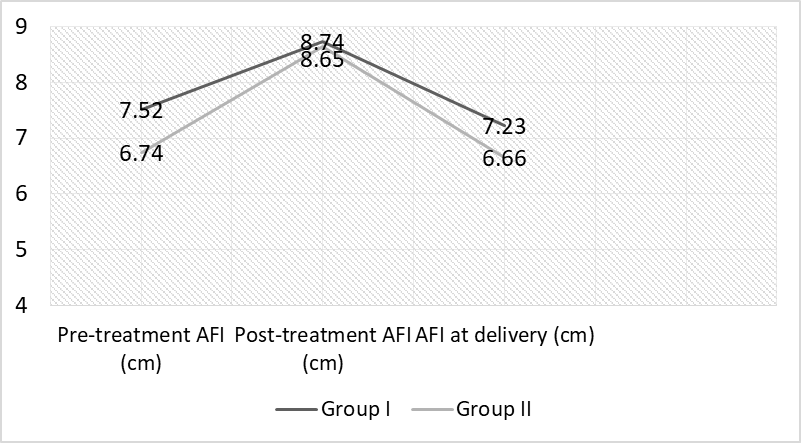
The average amniotic fluid index of patients at recruitment was 7.52 ± 0.88 cm and 6.74 ± 1.31 cm in Groups I and II respectively. Hebbar, Rai and Adiga recruited women with average AFI of 6.9 cm (4.7 cm to 7.4 cm) to study the effect of oral arginine and IV fructodex which was similar to the present study. In Group I (oral arginine only), the post treatment AFI was 8.47 ± 1.34 cm and in Group II (oral arginine + IV fructodex), it was 8.65 ± 1.54 cm. Both groups had significant increase in AFI after 1 week of treatment ([Table 1]).
After one week of treatment with only oral arginine, Group I showed an increase in AFI of 0.95 ± 1.11 cm, which was statistically significant. Sreedharan et al conducted studies by treating patients with oral arginine once a day, over an average period of 3 weeks.[12] They showed an increase in AFI of 2.03 ± 0.39 cm. Soni et al treated patients with oral arginine thrice a day for one week and had a significant increase in AFI of 3.33 cm per week.[11] The higher increase in post-treatment AFI in these studies can probably be due to an increase in duration and frequency of treatment.
In the present study, average increase in AFI was 1.87 ± 1.22 cm after 1 week of treatment with IV Fructodex with oral arginine in Group II, which was statistically significant. Nada showed an increase in AFI of 2.98 ± 0.8 cm and 2.64 ± 0.96 cm in patients treated with oral hydration and IV fluids respectively, 2 hours post treatment.[13]
In the study by Hebbar et al in 2018, 50 high risk women at an average gestational age of 33.4 weeks, were divided into two groups and treated with IV Fructodex or with oral arginine alone. They found a 1.8 cm increase in AFI in the group treated with oral arginine and a 2.5 cm increase in the group treated with IV fructodex. The patients were treated for an average period of 18.4 days.
In the present study, at the end of one week, individually, each modality of treatment showed a statistically significant rise in AFI at the end of 1 week of treatment. However, on an average, the increase in AFI in Group II over Group I was 0.92 cm higher. This can be attributed to the fact that IV hydration has a more direct effect on increasing maternal plasma volume and thus gives a better immediate result in improving AFI.
The average AFI at the time of delivery in Group I had decreased by 1.23 ± 1.97 cm and in Group II by 1.99 ± 2.15 cm. ([Table 1]). Group II had a higher mean reduction in AFI by the time of delivery than Group I, and this was statistically significant ([Figure 1]).
Both Group I and II showed significant a decrease in AFI from the end of treatment to the time of delivery. Similarly, in the study done by Nada Z., 64.7% of patients treated with oral hydration and 58.8% of patients treated with IV fluids had improvement in AFI. However, AFI returned to pre-treatment values within 48 hours in most patients and the rest reverted to pre-treatment values after 1 week.[13] Lorzadeh et al found that though there was a significant increase in AFI post treatment with IV fluids and this effect lasted for about 24 hours only.[14] This shows that increase in AFI occurs due to immediate increase in maternal plasma volume. The decrease in AFI, as the pregnancy progresses may be a part of normal physiological change seen or because the cause of oligohydramnios is not being treated.
The average gestational age of the patients at recruitment for the study was 33 weeks in Group I and II. In Group I, the pregnancy was prolonged for an average period of 4.48 weeks and in Group II, for 4.24 weeks. The duration of prolongation of pregnancy was found to be significant in both the groups.
Hebbar et al, Soni et al and Sharma et al all had an average increase in duration of pregnancy of only 2.9 weeks. In comparison, in the present study, the pregnancy was prolonged for an average period of 4.48 weeks and 4.24 weeks in Group I and II respectively. This could be attributed to the fact that the above mentioned studies included pregnant women with or without complications.[7], [11], [15]
Secondary outcomes like mean increase in fetal weight, mode of delivery, post-natal assessment of APGAR and NICU admission were as in [Table 2]. They were not found to be statistically significant. Ten (16.7%) babies in Group I and 9 (15%) babies in Group II were admitted in NICU for respiratory distress. This data was not found to be statistically significant.
In comparison to the present study, other studies had a higher rate of caesarean section, lower postnatal APGAR scores and higher frequency of NICU admission, as they had recruited high risk patients with hypertensive disorders and IUGR.[7], [11], [15]
In the present study, in Group I, majority of the pregnant women had no major difficulties due to the treatment or any side effects. Minor side effects like nausea and vomiting were seen. In Group II, thrombophlebitis, and chills due to the administration of IV fluids was seen, though not very significant, however, none of the patients had fluid overload.
Conclusion
This study concludes that the treatment with oral arginine alone and oral arginine and IV fructodex for one week produces an immediate increase in AFI of 0.9 cm and 1.8 cm respectively. The average duration of prolongation of pregnancy was 4.24 weeks in both the groups. Both groups had similar maternal and fetal outcomes, in terms of mode of delivery, APGAR score and NICU admission. However, AFI at delivery was lower in the group treated with IV Fructodex. This indicates that despite a higher immediate increase in AFI, patients reverted to pre-treatment AFI levels at the time of delivery, showing that the increase in AFI post treatment was transient. In view of added discomfort and logistic difficulty in administering IV fructodex, we suggest that it may be more efficient to manage moderate idiopathic oligohydramnios in pregnant women far from term, with continuous oral arginine. In the future, we suggest that studies can be done to compare the changes in AFI post various duration of treatment with oral arginine only. More studies can also be done to observe the effects of IV fructodex on patients with severe oligohydramnios.
Source of Funding
None.
Conflict of Interest
The authors guarantee that there were no conflicts of interest in this study.
References
- Cunningham F. . Williams obstetrics. 2018. [Google Scholar]
- . Antepartum fetal surveillance. Practice Bulletin 145. . 2014;124:182-92. [Google Scholar]
- Gabbe S. . Obstetrics: normal and problem pregnancies. 2017. [Google Scholar]
- Banks E, Miller D. Perinatal risks associated with borderline amniotic fluid index. Am J Obstet Gynecol. 1999;180(6):1461-3. [Google Scholar]
- Bhide A, Arulkumaran S, Damania K, Daftary S, Arias F. . Arias’ practical guide to high-risk pregnancy and delivery: a South Asian perspective. 2015. [Google Scholar]
- Shree P, Mittal N, Kanti V, Vishwakarma S. Role of intravenous amino acid infusion in cases of oligohydramnios and its effect on amniotic fluid index and fetal weight gain. Int J Reprod Contracept Obstet Gynecol. 2016;5(8):2804-9. [Google Scholar]
- Hebbar S, Rai L, Adiga P. Maternal hydration and L-arginine supplementation improves liquor volume in patients with decreased liquor and prolongs pregnancy. Med J Dr Patil Univ. 2014;7(4):429-34. [Google Scholar]
- Shivkumar P, Tayade S, Pramodkumar, Tayade A, Bagde N, Bagde M. The role of intravenous hydration and amino infusion in intrauterine growth restriction and oligohydramnios. Int J Biol Med Res. 2011;2(4):1078-83. [Google Scholar]
- James D. . High risk pregnancy management options. 2011. [Google Scholar]
- Palmer R, Ashton D, Moncada S. Vascular endothelial cells synthesize nitric oxide from L-arginine. Nature. 1988;333(6174):664-6. [Google Scholar]
- Soni A, Garg S, Patel K, Patel Z. Role of l-Arginine in Oligohydramnios. J Obstet Gynaecol India. 2016;66(1):279-83. [Google Scholar]
- Sreedharan R, Jajoo S. Effect of L-arginine on amniotic fluid index in oligohydramnios. Int J Reprod Contracept Obstet Gynecol. 2013;2(1):80-2. [Google Scholar]
- Nada Z. Oral and Intravenous Maternal Hydration in third trimester Idiopathic Oligohydramnios:Effects and Duration. IOSR J Nurs Nd Health Sci. 2015;4(5):22-5. [Google Scholar]
- Lorzadeh N, Kazemirad S, Lorzadeh M, Najafi S. Comparison of the Effect of Oral and Intravenous Fluid Therapy on Women with Oligohydramnios. Res J Obstet Gynecol. 2008;1(1):25-9. [Google Scholar]
- Sharma A, Dashora S, Sharma R, Chandra K, Gunawat M. To Study The Effect of L-Arginine in Oligohydramnios To Improve Perinatal Outcome. IOSR J Dent Med Sci. 2017;16(4):16-9. [Google Scholar]